Nurse · Discharge letter · Grade B worked sample
Nurse — Discharge to Community Nurse (Grade B Sample)
Worked example showing a Grade B discharge letter from a hospital nurse to a community nurse. Use this to model content, organisation and clinical detail.
In short
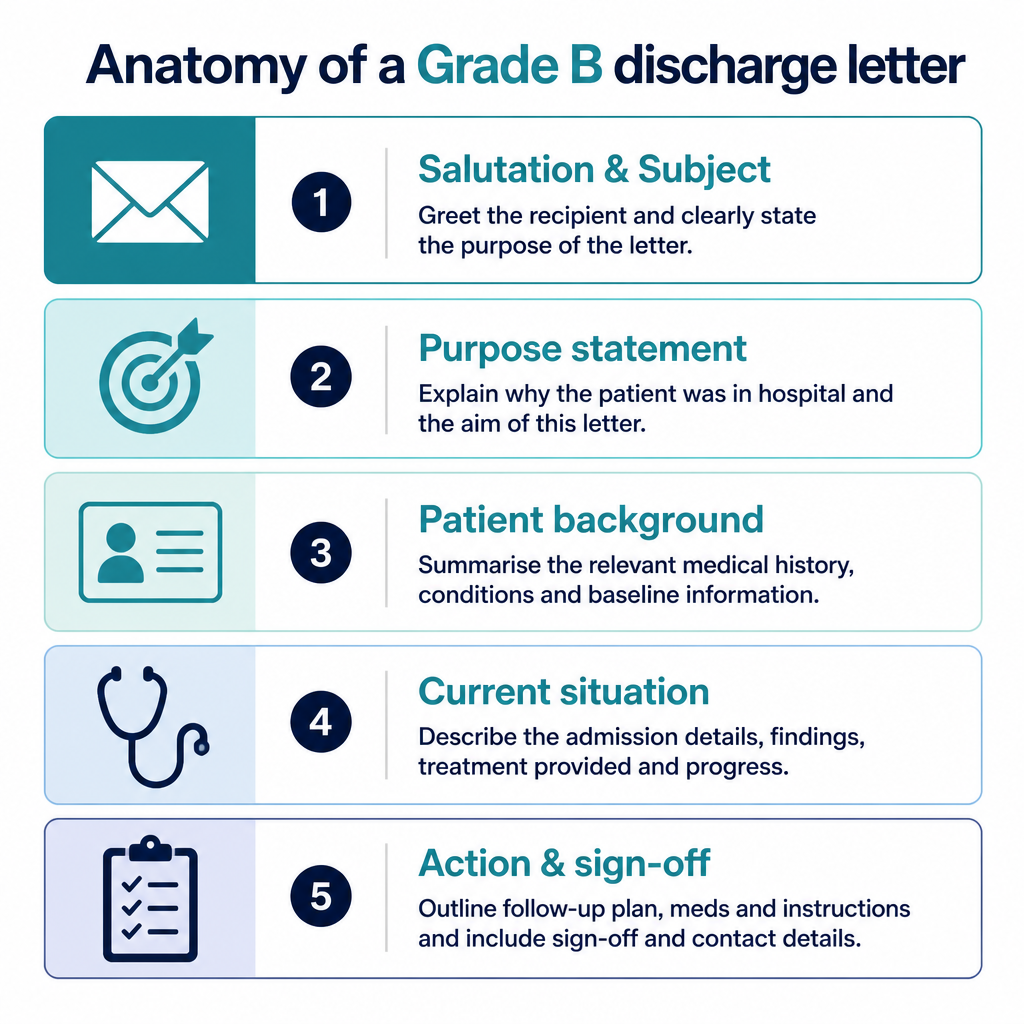
- →Clear purpose statement with patient identifiers and discharge date.
- →Summarises treatment, current status and exact medication instructions.
- →Specifies daily community nursing tasks, monitoring parameters and follow-up.
The case notes
The OET writing task you would receive in this scenario.
Anatomy of this letter
The Grade B sample letter
A complete worked example written to score Grade B (350+) against all six criteria.
Ms Patel
Community Nurse
16 May 2026
Discharge: Mr John Reid (DOB 02/04/1948)
Dear Ms Patel,
I am writing to inform you that Mr John Reid (DOB 02/04/1948) was discharged from our ward on 15 May 2026 following admission for left lower leg cellulitis. He was admitted on 10 May and responded well to initial intravenous antibiotics.
Treatment summary: IV flucloxacillin 1 g 6‑hourly for 48 hours, then oral flucloxacillin 500 mg four times daily to complete a seven‑day course. He is afebrile and reported reduced pain; mobility is independent with a stick. Regular medications to continue: amlodipine 5 mg once daily and simvastatin 20 mg nocte.
Nursing requirements for community care: please visit daily for 7 days to perform simple dry dressing changes to the left lower leg, monitor wound for increasing erythema, spreading cellulitis, drainage or new fever, and record observations (temperature, pain score, mobility). Administer oral antibiotics as prescribed and ensure paracetamol 1 g PRN for pain is given if required.
Please contact the ward if you note deterioration or if concerns persist; GP review is arranged in 7 days. If you need further information about meds or wound status, telephone the unit and ask for the nurse in charge.
Yours sincerely, A. Walker, Nurse
Why this letter scores Grade B — annotation by annotation
Each highlighted phrase maps to one of the six OET writing criteria.
| Phrase from the letter | Criterion | Examiner comment |
|---|---|---|
| "I am writing to inform you that Mr John Reid (DOB 02/04/1948) was discharged from our ward on 15 May 2026" | Purpose | Clear opening purpose with full patient identifiers and discharge date supports immediate reader orientation. |
| "IV flucloxacillin 1 g 6‑hourly for 48 hours, then oral flucloxacillin 500 mg four times daily to complete a seven‑day course" | Content | Specific medication names, dosages and duration give the community nurse actionable treatment information. |
| "He is afebrile and reported reduced pain; mobility is independent with a stick" | Conciseness & Clarity | Brief clinical status update summarises key observations without extraneous detail. |
| "please visit daily for 7 days to perform simple dry dressing changes" | Organisation & Layout | Direct instruction listed under nursing requirements makes the required actions easy to find and follow. |
| "monitor wound for increasing erythema, spreading cellulitis, drainage or new fever" | Genre & Style | Appropriate clinical tone and explicit escalation signs guide the community nurse on when to seek further input. |
| "Please contact the ward if you note deterioration or if concerns persist" | Language | Polite imperative phrasing with clear contact action; could be improved with direct contact number for speed. |
| "Regular medications to continue: amlodipine 5 mg once daily and simvastatin 20 mg nocte" | Content | Lists ongoing meds to prevent omission after discharge; including times aids administration. |
Criterion-by-criterion score breakdown
| Criterion | Score | Why |
|---|---|---|
| Purpose | 3 / 3 | Purpose is explicit and patient identifiers are provided, enabling clear intent. |
| Content | 5 / 7 | Most key clinical details and nursing actions are included but could add specific contact phone number and dressing materials. |
| Conciseness & Clarity | 5 / 7 | Information is generally succinct and clear though one sentence could be split for greater clarity. |
| Genre & Style | 5 / 7 | Professional tone with appropriate clinical language; slight improvements in explicit escalation pathways would raise score. |
| Organisation & Layout | 6 / 7 | Well structured with purpose, summary and clear nursing actions; headings or bulleting would improve rapid scanning. |
| Language | 5 / 7 | Mostly accurate grammar and vocabulary; a few opportunities to use more precise terms and contact details. |
5 Nurse pitfalls to avoid
1. Omitting clear patient identifiers or discharge date
Fix: Always open with full name, DOB and discharge date in the first sentence.
2. Vague medication instructions without dose or duration
Fix: Include exact drug names, doses, frequency and total duration.
3. Failing to state specific nursing tasks or frequency
Fix: List required actions (e.g., dressing changes daily for 7 days) clearly and early.
4. Overloading letter with irrelevant ward details
Fix: Limit to information the community nurse needs to provide care post-discharge.
5. No escalation guidance or contact details
Fix: Provide signs to watch for and a direct contact route for concerns.
2026 update
What changed in 2026 for Nurse letters
From 2026, marking is stricter: examiners expect precise, relevant content and explicit nursing actions. Ambiguity in tasks or medication details now leads to greater penalty.
As a nurse writing discharge letters, state exact doses, durations, dressing regimes and monitoring parameters. Use short, direct sentences, label required actions, and include escalation steps and contact routes to meet the higher standard for clarity and utility in community care settings. Documentation must be immediately actionable.
Frequently asked questions
How long should a nurse discharge letter be for community care?
Aim for a concise letter of around 180–220 words focusing on purpose, key treatment, nursing tasks and escalation instructions.
What patient identifiers must I include?
Include full name, date of birth and a local identifier such as NHS number or hospital ID for unambiguous identification.
How should I present medication information?
List drug name, dose, route, frequency and duration; note which medicines to continue and which were stopped.
Do I need to supply contact details?
Yes. Give a clear contact route (ward phone or nurse in charge) and when to use it for urgent issues.
What escalation information is expected?
Specify signs to watch for (e.g., increasing erythema, fever, drainage) and state to contact the ward or GP if they occur.
How formal should the tone be?
Use a professional, concise clinical register appropriate for interprofessional communication; avoid colloquialisms and speculation.
Keep learning
Relevant scoring criteria
Related guides
Want Dr Mariam to mark YOUR nurse letter against all six criteria?
See OET Writing Correction packs →