Doctor (GP) · Transfer letter · Grade B worked sample
Doctor (GP) Transfer letter to consultant (Grade B Sample)
Worked example of a Grade B transfer letter from a GP to a consultant, showing the level expected in OET writing for this scenario.
In short
- →Refer a 67-year-old man with 3-week exertional chest tightness and multiple vascular risk factors.
- →Include concise history, current meds and exam findings, and request cardiology assessment and investigations.
- →State urgency, safety-netting, and clear actions for the receiving consultant to consider.
The case notes
The OET writing task you would receive in this scenario.
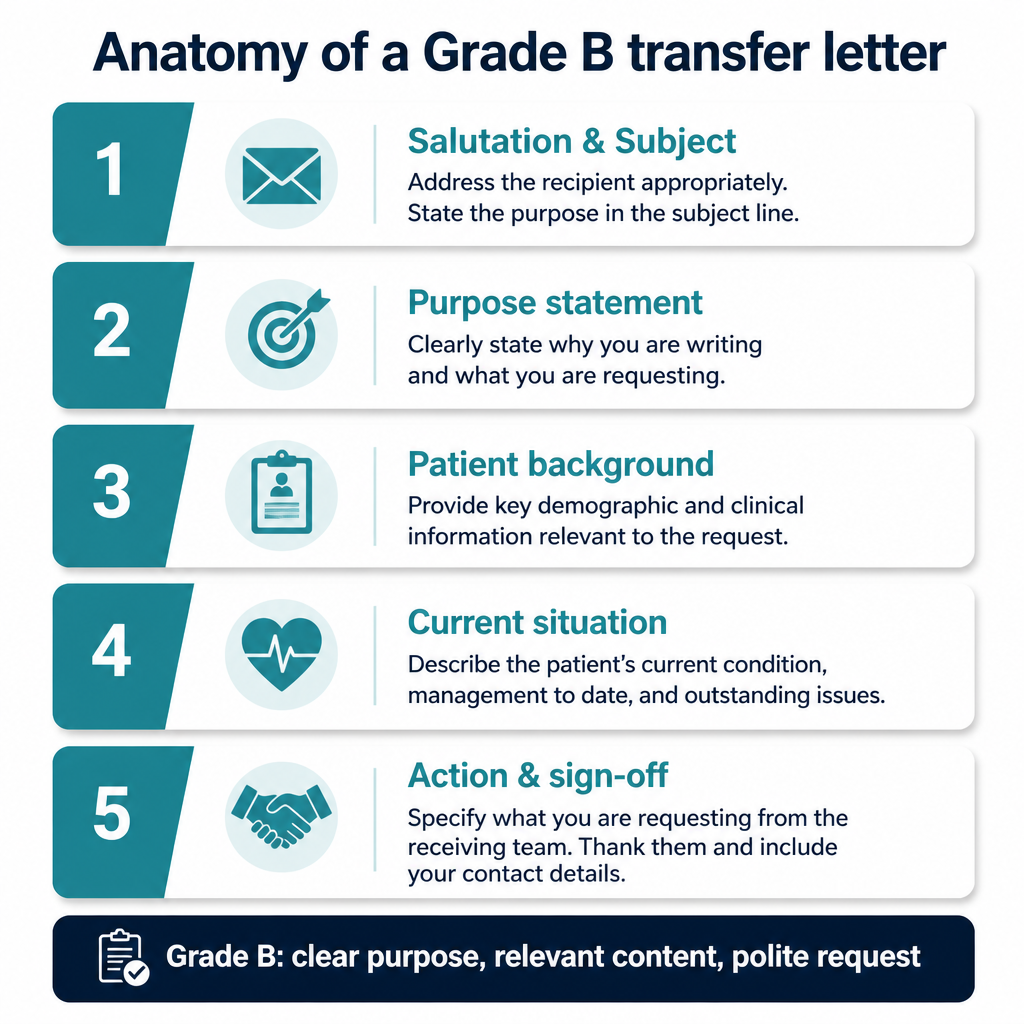
Anatomy of this letter
The Grade B sample letter
A complete worked example written to score Grade B (350+) against all six criteria.
Dr Smith
Consultant Cardiologist
16/05/2026
Referral: Mr J. Khan — exertional chest pain, possible angina
Dear Dr Smith,
I am writing to refer Mr J. Khan, a 67-year-old man, for cardiology assessment following three weeks of exertional central chest tightness that is relieved by rest. He has type 2 diabetes, hypertension and hyperlipidaemia, and is an ex-smoker.
On examination today his blood pressure was 142/86 mmHg and heart rate 78 bpm. A 12-lead ECG performed in practice showed sinus rhythm without acute ischaemic change. Recent blood tests show HbA1c 67 mmol/mol. Current medications are metformin 1 g twice daily, ramipril 5 mg daily, atorvastatin 40 mg nocte and clopidogrel was not indicated; I have commenced aspirin 75 mg daily after discussion. He reports no syncope, palpitations or resting chest pain.
Could you please assess for stable angina and advise on appropriate investigations — preferably exercise ECG or CT coronary angiography as you deem appropriate — and management including consideration of anti-anginal therapy. I would be grateful for prioritisation given his multiple cardiac risk factors. Please advise any changes to medications and secondary prevention.
If his symptoms worsen (pain at rest, prolonged or associated breathlessness) he will return to the practice or attend A&E. I enclose copies of ECG and blood results.
Yours sincerely, Dr A. Walker, MBBS
Why this letter scores Grade B — annotation by annotation
Each highlighted phrase maps to one of the six OET writing criteria.
| Phrase from the letter | Criterion | Examiner comment |
|---|---|---|
| "I am writing to refer Mr J. Khan, a 67-year-old man, for cardiology assessment" | Purpose | Clearly states the reason for writing and the recipient service, establishing purpose immediately. |
| "three weeks of exertional central chest tightness that is relieved by rest" | Content | Concise presentation of primary symptom with timeframe and relieving factor, relevant for differential diagnosis. |
| "Current medications are metformin 1 g twice daily, ramipril 5 mg daily, atorvastatin 40 mg nocte" | Content | Provides key medication names and dosages necessary for specialist decision-making and safety checks. |
| "Could you please assess for stable angina and advise on appropriate investigations" | Genre & Style | Polite, professional request for action with suggested investigations, fitting the referral genre. |
| "Please advise any changes to medications and secondary prevention" | Conciseness & Clarity | Direct request for specific outcomes from the consultant; concise but could state a preferred timeframe. |
| "If his symptoms worsen (pain at rest, prolonged or associated breathlessness) he will return" | Organisation & Layout | Safety-netting appears at the end, logically placed to conclude the clinical priorities for the receiving team. |
| "A 12-lead ECG performed in practice showed sinus rhythm without acute ischaemic change" | Language | Uses accurate clinical terminology and concise sentence structure suitable for professional readers. |
Criterion-by-criterion score breakdown
| Criterion | Score | Why |
|---|---|---|
| Purpose | 2 / 3 | Purpose is stated clearly but could specify urgency level more explicitly. |
| Content | 6 / 7 | Most relevant clinical details, medications and investigations included; minor omissions (e.g. smoking pack-years). |
| Conciseness & Clarity | 5 / 7 | Information is mostly concise and clear but occasional phrases could be tightened for precision. |
| Genre & Style | 5 / 7 | Professional tone and appropriate requests present; could better emphasise urgency and next steps. |
| Organisation & Layout | 6 / 7 | Logical paragraphing and clear flow from history to request and safety-netting. |
| Language | 6 / 7 | Accurate clinical language and varied sentence structures with only minor grammatical slips. |
5 Doctor (GP) pitfalls to avoid
1. Vague purpose without specifying referral reason or urgency
Fix: Begin with a clear, single-sentence purpose and state urgency (routine/urgent).
2. Omitting exact medication names or doses
Fix: List current drugs with dosages and any allergies for safety.
3. Including irrelevant social details
Fix: Stick to clinically relevant history affecting diagnosis or management.
4. Unclear request for investigations or follow-up
Fix: Specify desired investigations and what you want the consultant to do.
5. Poor organisation causing important details to be missed
Fix: Use short paragraphs: purpose, history, current status, request, safety-netting.
2026 update
What changed in 2026 for Doctor (GP) letters
The 2026 stricter scoring regime places greater emphasis on an explicit, immediate purpose and tightly focused content.
For a GP writing a transfer letter, that means state clearly why you are referring and the urgency, include only relevant findings (accurate meds, key vitals, recent tests), and end with a specific, actionable request. Excess background or vague language risks lower scores under the new expectations; prioritise clinical relevance and clear, professional requests to the consultant.
Frequently asked questions
How should I state urgency in a transfer letter?
Explicitly label urgency (routine, urgent, urgent—same/next week) in the first paragraph and repeat if necessary in the request.
What medications must always be included?
Include current prescriptions with doses, recent changes, and any allergies or anticoagulants that affect investigations.
How long should the referral letter be?
Aim for one page: concise paragraphs that cover purpose, key history, current findings, and a clear request with safety-netting.
Do I need to suggest specific investigations?
Yes when appropriate; recommend investigations (e.g. exercise ECG, CTCA) but remain open to specialist discretion.
Where should safety-netting appear?
Place safety-netting at the end of the letter so the receiving clinician knows what to advise if the condition worsens.
How formal should the tone be?
Maintain a professional, courteous tone—polite requests, clinical language and no slang or contractions.
Keep learning
Relevant scoring criteria
Related guides
Want Dr Mariam to mark YOUR doctor (gp) letter against all six criteria?
See OET Writing Correction packs →