Doctor (GP) · Referral letter · Grade B worked sample
Doctor (GP) Referral to specialist — Colorectal (Grade B Sample)
Worked example showing a Grade B referral letter from a GP to a specialist colorectal consultant for suspected colorectal malignancy.
In short
- →Refer promptly with a clear urgent purpose statement and relevant timelines.
- →Include brief history, current meds, recent bloods and FIT results.
- →Request specific investigation (colonoscopy/CT colonography) and state patient availability.
The case notes
The OET writing task you would receive in this scenario.
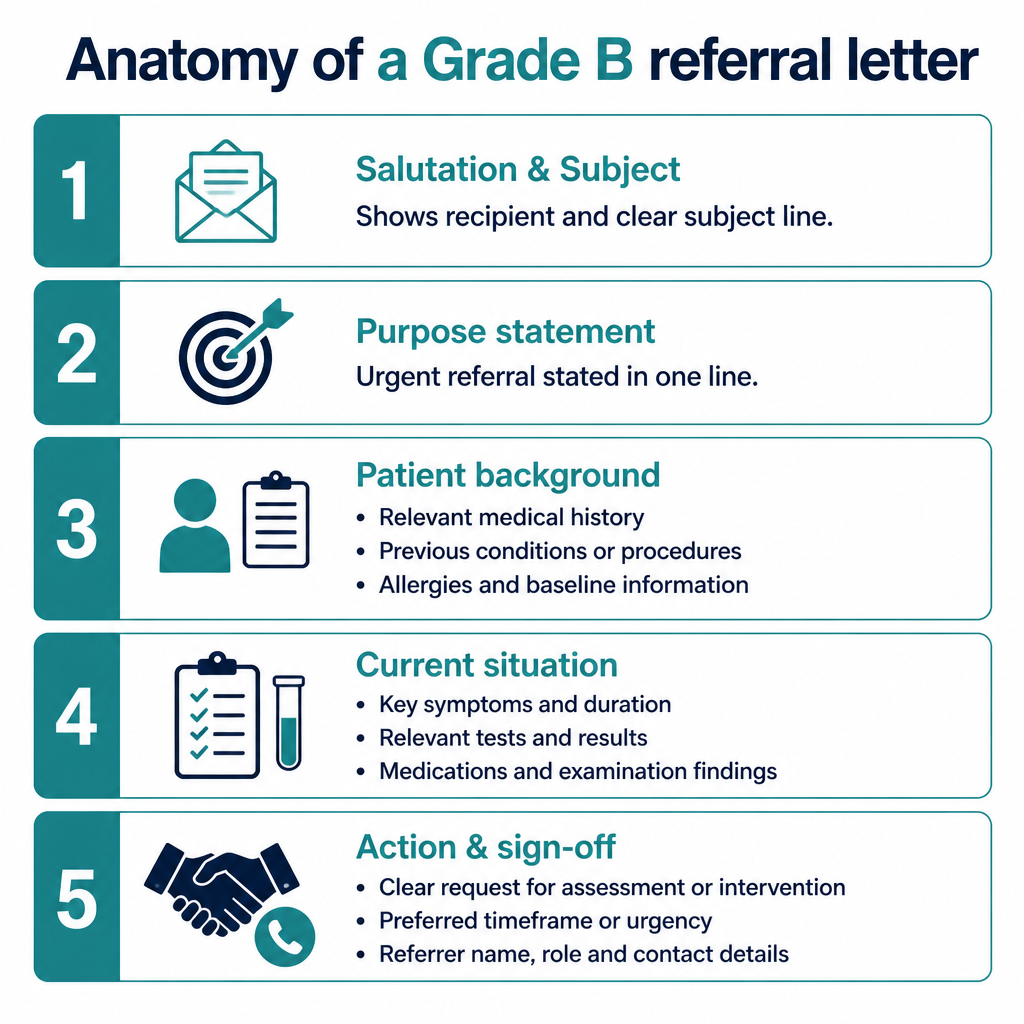
Anatomy of this letter
The Grade B sample letter
A complete worked example written to score Grade B (350+) against all six criteria.
Dr Smith
Consultant Colorectal Surgeon
16 May 2026
Urgent referral: Mr R J Brown — iron-deficiency anaemia and PR bleeding
Dear Dr Smith,
I am referring Mr Robert J Brown (DOB 03/02/1958, NHS 123 456 7890) for urgent colorectal assessment. He presents with progressive iron-deficiency anaemia and intermittent rectal bleeding, and I am concerned this warrants investigation under the suspected cancer pathway.
Over the past three months he reports bright rectal bleeding approximately once weekly, looser bowel habit and an unintentional weight loss of 6 kg. His past medical history includes hypertension and osteoarthritis; he had a colonoscopy in 2014 with no significant findings. Current medications: aspirin 75 mg daily, atorvastatin 20 mg nocte and lisinopril 10 mg mane. He is not anticoagulated and is a former smoker.
Investigations in primary care (10 May 2026): Hb 95 g/L, MCV 72 fL, ferritin 8 µg/L. Faecal immunochemical test (FIT) is positive. Abdominal examination is unremarkable and he is haemodynamically stable. I have started oral ferrous sulfate 200 mg twice daily with good tolerance.
Please would you arrange urgent endoscopic assessment (colonoscopy) and CT colonography if colonoscopy is contraindicated. I have attached blood results and FIT. Mr Brown is available for weekday appointments; please contact the surgery for further information or to discuss interim management.
Yours sincerely, Dr A. Walker, MBBS
Why this letter scores Grade B — annotation by annotation
Each highlighted phrase maps to one of the six OET writing criteria.
| Phrase from the letter | Criterion | Examiner comment |
|---|---|---|
| "I am referring Mr Robert J Brown ... for urgent colorectal assessment." | Purpose | Clear immediate purpose and urgency signalled at the opening — aligns with what the specialist needs to know first. |
| "Over the past three months he reports bright rectal bleeding approximately once weekly, looser bowel habit and an unintentional weight loss of 6 kg." | Content | Relevant history summarised concisely with duration and red-flag symptoms to justify urgent referral. |
| "Current medications: aspirin 75 mg daily, atorvastatin 20 mg nocte and lisinopril 10 mg mane." | Conciseness & Clarity | Medication list is brief, uses standard abbreviations and places key anticoagulant status beside it for quick review. |
| "Investigations in primary care (10 May 2026): Hb 95 g/L, MCV 72 fL, ferritin 8 µg/L. Faecal immunochemical test (FIT) is positive." | Genre & Style | Concise presentation of results in clinical units supports specialist triage and reflects professional register. |
| "Please would you arrange urgent endoscopic assessment (colonoscopy) and CT colonography if colonoscopy is contraindicated." | Organisation & Layout | Specific request is placed at the close of the letter, making the desired action easy to locate and act on. |
| "I have started oral ferrous sulfate 200 mg twice daily with good tolerance." | Content | Includes current treatment started in primary care, which is relevant to interim management and planning. |
| "Mr Brown is available for weekday appointments; please contact the surgery for further information or to discuss interim management." | Language | Polite, actionable closing with availability details; phrasing is clear but could include specific dates to improve precision. |
Criterion-by-criterion score breakdown
| Criterion | Score | Why |
|---|---|---|
| Purpose | 3 / 3 | Purpose is explicit and urgent, stated immediately in the opening sentence. |
| Content | 6 / 7 | Includes key history, medications, investigations and interim treatment, but minor details (e.g. exact dates of prior colonoscopy) could be added. |
| Conciseness & Clarity | 6 / 7 | Information is concise and clinically prioritised; could be marginally tighter in one or two sentences. |
| Genre & Style | 6 / 7 | Professional clinical register is maintained and the tone suits a GP-to-consultant referral. |
| Organisation & Layout | 6 / 7 | Logical paragraphing and a clear request at the end aid quick reading and action by the specialist. |
| Language | 5 / 7 | Generally accurate grammar and vocabulary; slight room for improved precision and avoidance of minor abbreviations. |
5 Doctor (GP) pitfalls to avoid
1. Failing to state urgency or referral pathway
Fix: Begin with a one-line purpose stating urgency and suspected pathway (e.g. suspected cancer).
2. Omitting current anticoagulant or antiplatelet status
Fix: List aspirin/anticoagulants explicitly and note whether treatment is paused.
3. Providing excessive unrelated background
Fix: Limit history to relevant symptoms, duration and red flags only.
4. Not attaching or summarising recent test results
Fix: Include key values in the letter and attach full bloods/FIT results.
5. Vague or multiple unclear requests
Fix: Make one clear request (e.g. colonoscopy) and note alternatives (CT colonography) if needed.
2026 update
What changed in 2026 for Doctor (GP) letters
From 2026 the scoring emphasises immediate clarity of purpose and clinical relevance. As a GP writing referrals, you must state urgency and the suspected pathway in the opening line and prioritise only information that changes triage decisions.
You should attach key investigation results and give a specific, feasible request. Overlong narrative or non-essential history risks lowering marks under the stricter regime, so be concise and clinically precise while maintaining professional tone and organisation.
Frequently asked questions
What is the most important sentence in a referral letter?
The opening purpose statement: it must state who you are referring, the reason, and the urgency or pathway (eg suspected cancer).
How much investigation detail should I include?
Include key results (dates and units) that affect triage: Hb, ferritin, FIT. Attach full reports rather than overloading the letter.
Do I need to list all medications?
List current medications relevant to the referral, especially anticoagulants and antiplatelets, and note any recent changes.
How do I request urgent assessment?
State the request explicitly (eg urgent colonoscopy) and reference the suspected pathway; offer patient availability and attach supporting tests.
Is it acceptable to use abbreviations?
Use common clinical abbreviations (Hb, FIT) but avoid obscure acronyms; clarity for the specialist is essential.
How long should a GP referral letter be?
Aim for a concise letter of approximately 160–220 words, prioritising purpose, salient history, current findings and a clear request.
Keep learning
Relevant scoring criteria
Related guides
Want Dr Mariam to mark YOUR doctor (gp) letter against all six criteria?
See OET Writing Correction packs →