Doctor (GP) · Discharge letter · Grade B worked sample
Doctor (GP) — Discharge summary to GP (Grade B Sample)
This worked example shows a Grade B (band 6/7) discharge letter written by a GP to a patient’s usual GP. It demonstrates clear purpose and acceptable clinical detail with minor gaps.
In short
- →Short admission for community-acquired pneumonia; stabilised and discharged on oral antibiotics.
- →Continue amoxicillin 500 mg TDS for five days; monitor diabetes and review bloods in one week.
- →Arrange chest x-ray in six weeks and follow up with practice for vaccination and medication review.
The case notes
The OET writing task you would receive in this scenario.
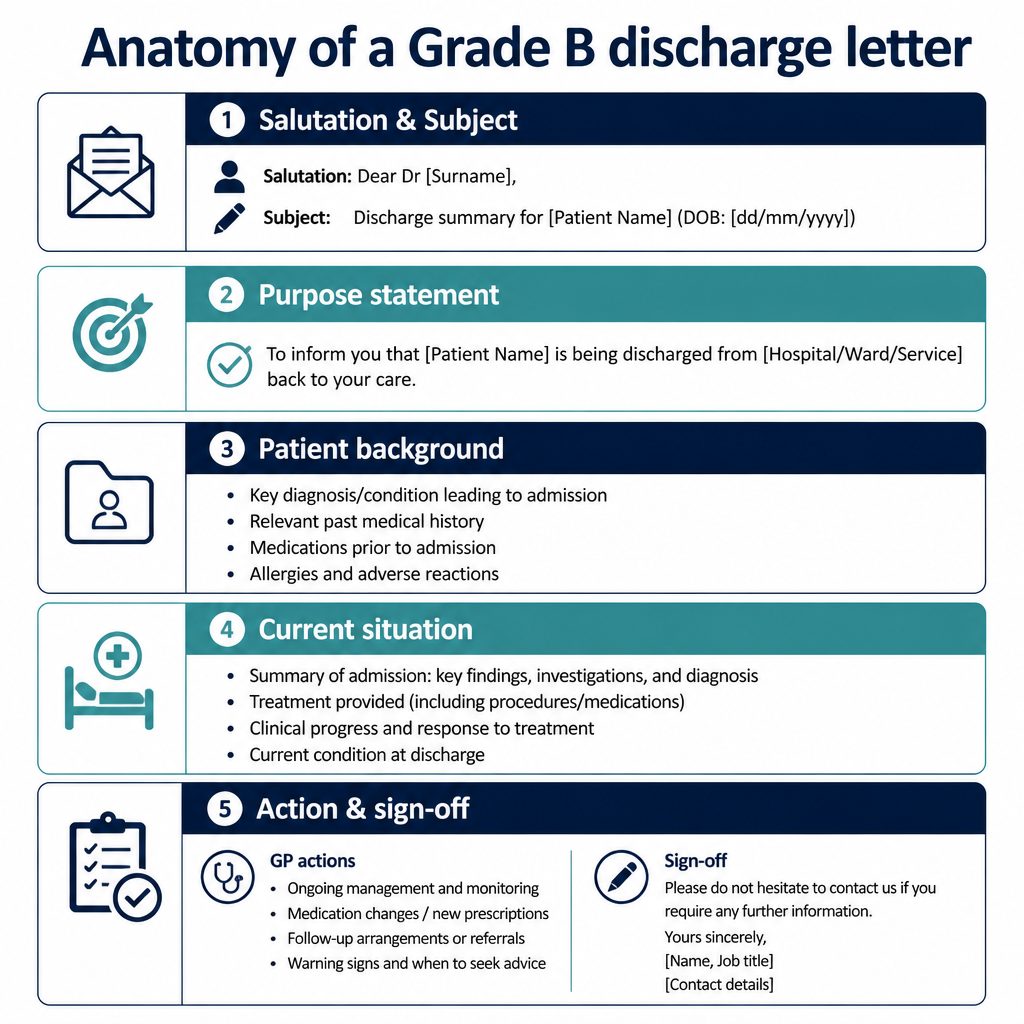
Anatomy of this letter
The Grade B sample letter
A complete worked example written to score Grade B (350+) against all six criteria.
Dr Smith
General Practitioner
16 May 2026
Discharge summary — Mr J. Khan (02/03/1957): community-acquired pneumonia
Dear Dr Smith,
I am writing to inform you that Mr J. Khan was admitted to the acute assessment unit on 12 May 2026 with community-acquired pneumonia and was discharged home on 15 May 2026.
On admission he had a productive cough, fever and increased breathlessness. Chest x-ray showed a right lower-zone consolidation. He received IV fluids and oral antibiotics; observations stabilised and he has been afebrile for 48 hours. CRP fell from 120 mg/L on admission to 24 mg/L at discharge and SpO2 is 95% on room air.
He is discharged on oral amoxicillin 500 mg three times daily to complete a five-day course. Continue his usual medications (metformin 500 mg twice daily, lisinopril 10 mg daily) and inhalers as before. Please review blood tests (FBC, U&E, CRP) in one week and review diabetic control. I would be grateful if you could arrange a chest x-ray in six weeks to ensure resolution and consider influenza and pneumococcal vaccination if appropriate.
If there are any concerns or deterioration, please contact the unit. Thank you for arranging ongoing care.
Yours sincerely, Dr A. Walker, MBBS
Why this letter scores Grade B — annotation by annotation
Each highlighted phrase maps to one of the six OET writing criteria.
| Phrase from the letter | Criterion | Examiner comment |
|---|---|---|
| "I am writing to inform you that Mr J. Khan was admitted to the acute assessment unit on 12 May 2026 with community-acquired pneumonia and was discharged home on 15 May 2026." | Purpose | Clear opening statement stating who, what, dates and the purpose; directly matches the GP’s information needs. |
| "Chest x-ray showed a right lower-zone consolidation." | Content | Relevant clinical finding given succinctly; would score better with brief comment on severity or scoring system. |
| "He received IV fluids and oral antibiotics; observations stabilised and he has been afebrile for 48 hours." | Conciseness & Clarity | Presents treatment and response clearly and concisely; avoids unnecessary detail while showing clinical improvement. |
| "He is discharged on oral amoxicillin 500 mg three times daily to complete a five-day course." | Genre & Style | Direct instruction about discharge medication appropriate for a clinical letter; style is professional and actionable. |
| "Please review blood tests (FBC, U&E, CRP) in one week and review diabetic control." | Organisation & Layout | Requests for GP action are grouped and clearly signposted, aiding handover and continuity of care. |
| "I would be grateful if you could arrange a chest x-ray in six weeks to ensure resolution and consider influenza and pneumococcal vaccination if appropriate." | Language | Polite phrasing and conditional language are appropriate, though 'ensure resolution' could be more specific (e.g. 'repeat CXR to confirm radiological resolution'). |
| "CRP fell from 120 mg/L on admission to 24 mg/L at discharge and SpO2 is 95% on room air." | Content | Includes objective measures showing improvement; helpful for GP assessment and risk stratification. |
Criterion-by-criterion score breakdown
| Criterion | Score | Why |
|---|---|---|
| Purpose | 3 / 3 | Purpose is explicit and immediate, stating admission and discharge dates and diagnosis. |
| Content | 5 / 7 | Includes key clinical details and actions but omits some specifics (e.g. microbiology results or allergy check detail). |
| Conciseness & Clarity | 5 / 7 | Information is generally concise and clear though a few phrases could be more precise. |
| Genre & Style | 5 / 7 | Professional clinical tone with appropriate requests; occasional hedging reduces directness. |
| Organisation & Layout | 5 / 7 | Logical paragraphing and clear action requests, but follow-up items could be numbered for greater clarity. |
| Language | 5 / 7 | Accurate medical language and correct tense use; minor room for improved lexical precision. |
5 Doctor (GP) pitfalls to avoid
1. Vague purpose statement.
Fix: Open with a single sentence stating admission dates, diagnosis and reason for the letter.
2. Missing explicit GP actions.
Fix: State required follow-up tests and medication reviews with timeframes.
3. Overly long treatment descriptions.
Fix: Summarise interventions and give key results rather than step-by-step notes.
4. Unclear medication instructions.
Fix: Provide drug name, dose, frequency and duration for discharge prescriptions.
5. No evidence of improvement or objective data.
Fix: Include brief objective measures (CRP, SpO2, temperature) to support discharge decision.
2026 update
What changed in 2026 for Doctor (GP) letters
The 2026 stricter scoring regime emphasises unmistakable purpose and complete, relevant content. For a GP writing a discharge letter this means opening with precise admission and diagnosis details, including concise clinical data and unambiguous requests for follow-up.
Markers now expect clearer directives: specific tests, timeframes and exact medication instructions. Language must be economical and clinically precise; hedging and missing particulars are more likely to reduce the band to B under the new standards.
Frequently asked questions
How long should a GP discharge summary be?
Aim for 180–220 words: concise but complete, with purpose, key treatment, discharge meds, and explicit follow-up actions.
What is the most important sentence in the letter?
The opening purpose sentence — it must state who, admission dates and the diagnosis to orient the receiving GP immediately.
How do I show clinical improvement succinctly?
Give one or two objective measures (e.g. CRP, SpO2) and a simple statement such as 'afebrile for 48 hours'.
What level of medication detail is required?
Include drug name, dose, frequency and duration for all discharge prescriptions; note any medication changes from baseline.
Should I request investigations?
Yes — specify the test, timing (e.g. 'in one week') and the purpose (e.g. 'to monitor CRP and renal function').
How formal should tone be?
Use a professional clinical register: polite but direct, avoiding colloquialisms and unnecessary hedging.
Keep learning
Relevant scoring criteria
Related guides
Want Dr Mariam to mark YOUR doctor (gp) letter against all six criteria?
See OET Writing Correction packs →