Dentist · Referral letter · Grade B worked sample
Dentist Referral to Oral Surgeon — Impacted Lower Molar (Grade B Sample)
Worked example of a Grade B (band 6/7) referral letter from a general dentist to an oral and maxillofacial surgeon for surgical removal of an impacted lower third molar.
In short
- →Clear purpose and referral urgency for recurrent pericoronitis and impaired mouth opening.
- →Relevant medical history, radiographic finding and current analgesia included.
- →Request assessment for removal and advice on pre-op antibiotics and peri‑operative optimisation.
The case notes
The OET writing task you would receive in this scenario.
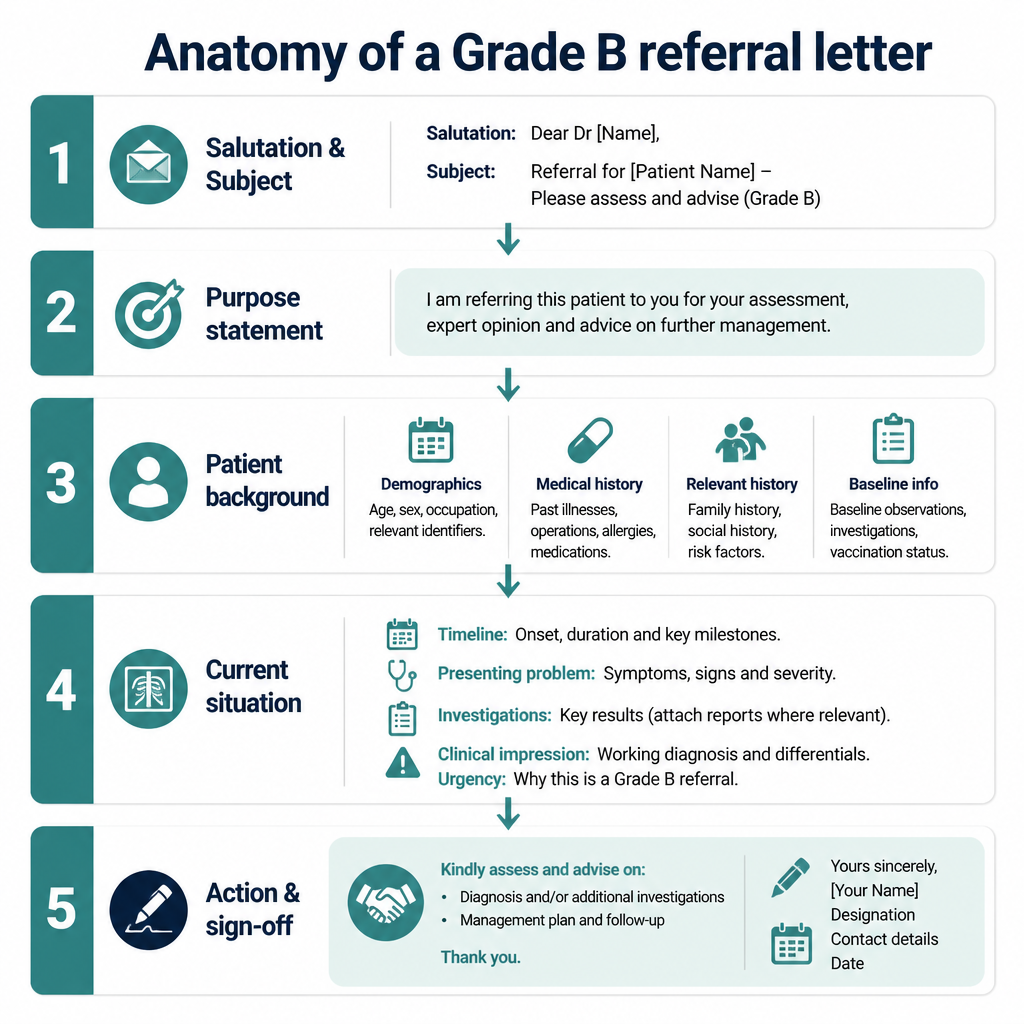
Anatomy of this letter
The Grade B sample letter
A complete worked example written to score Grade B (350+) against all six criteria.
Dr Smith
Consultant Oral and Maxillofacial Surgeon
16/05/2026
Referral: LR8 impacted mandibular third molar — Mr J.T.
Dear Dr Smith,
I am referring Mr J.T. (DOB 12/04/1978) for assessment and surgical removal of the lower left impacted mandibular third molar (LR8) following recurrent pericoronitis and failed conservative management. He has had three episodes in the past six months causing significant pain and intermittent trismus; local debridement and chlorhexidine rinse have provided only temporary relief.
Relevant medical history includes well-controlled type 2 diabetes (metformin 500 mg twice daily), hypertension managed with lisinopril 10 mg daily, and no known drug allergies. He is a current smoker (10 cigarettes/day) and has a BMI of 29. Most recent blood tests (2 months ago) show HbA1c 54 mmol/mol; BP 132/78.
Current problems are ongoing pain rated 6/10, left lower jaw swelling and reduced mouth opening approximately 25 mm. Panoramic radiograph shows a mesioangular impaction with a small pericoronal radiolucency; no obvious root resorption. Analgesia is ibuprofen 400 mg tds PRN and paracetamol 1 g qds PRN; chlorhexidine 0.12% mouthwash twice daily.
Please assess for removal under local anaesthesia with or without intravenous sedation, or under general anaesthesia if you deem appropriate. Given his diabetes and smoking, advise whether pre‑operative antibiotics are indicated and whether glycaemic control or smoking cessation support is required prior to surgery. Please contact me with proposed timing and any pre‑operative requirements; the patient is available for pre‑assessment at short notice.
Yours sincerely, A. Walker, Dentist
Why this letter scores Grade B — annotation by annotation
Each highlighted phrase maps to one of the six OET writing criteria.
| Phrase from the letter | Criterion | Examiner comment |
|---|---|---|
| "I am referring Mr J.T. (DOB 12/04/1978) for assessment and surgical removal of the lower left impacted mandibular third molar (LR8) following recurrent pericoronitis and failed conservative management." | Purpose | Explicit, immediate purpose stated with patient identifiers and reason; could improve by adding requested urgency level (e.g. 'urgent'). |
| "He has had three episodes in the past six months causing significant pain and intermittent trismus; local debridement and chlorhexidine rinse have provided only temporary relief." | Content | Provides clinical context and prior treatment, which supports the request for surgical assessment. |
| "Relevant medical history includes well-controlled type 2 diabetes (metformin 500 mg twice daily), hypertension managed with lisinopril 10 mg daily, and no known drug allergies." | Conciseness & Clarity | Concise summary of comorbidities and medications; presents essential pre‑operative information without extraneous detail. |
| "Panoramic radiograph shows a mesioangular impaction with a small pericoronal radiolucency; no obvious root resorption." | Content | Includes a key radiographic finding relevant to surgical planning; succinct and clinically useful. |
| "Please assess for removal under local anaesthesia with or without intravenous sedation, or under general anaesthesia if you deem appropriate." | Genre & Style | Polite professional request offering options and deferring technical decisions appropriately to the specialist. |
| "Given his diabetes and smoking, advise whether pre‑operative antibiotics are indicated and whether glycaemic control or smoking cessation support is required prior to surgery." | Organisation & Layout | Clear request for specific pre‑operative advice, placed logically at the end of the clinical summary to guide the surgeon's response. |
| "Please contact me with proposed timing and any pre‑operative requirements; the patient is available for pre‑assessment at short notice." | Language | Direct closing sentence using polite professional language; provides next steps and availability, facilitating coordination. |
Criterion-by-criterion score breakdown
| Criterion | Score | Why |
|---|---|---|
| Purpose | 3 / 3 | Purpose is explicit and appropriate with patient identifiers and reason for referral. |
| Content | 5 / 7 | Includes most relevant clinical information and radiographic finding, but could specify urgency and last blood results date. |
| Conciseness & Clarity | 5 / 7 | Information is generally concise and unambiguous though a few sentences could be tightened. |
| Genre & Style | 5 / 7 | Professional tone and appropriate requests; occasional phrasing could be more directive about expectations. |
| Organisation & Layout | 5 / 7 | Logical paragraphing and clear final requests, but urgency and follow‑up plan could be more prominent. |
| Language | 5 / 7 | Generally accurate clinical language with minor stylistic slips; vocabulary and grammar are sufficient for purpose. |
5 Dentist pitfalls to avoid
1. Omitting radiographic findings
Fix: Include a brief description of the radiograph (e.g. mesioangular impaction, pericoronal radiolucency).
2. Failing to state current analgesia and regular medications
Fix: List analgesics and regular meds with dosages to inform peri‑operative planning.
3. Not asking a clear action or timescale
Fix: End with a direct request (assessment, timing, pre‑op requirements) and patient availability.
4. Including irrelevant social details
Fix: Keep social history concise and only include if it affects surgery (smoking, mobility).
5. Using vague language about risks or prior treatments
Fix: State specific prior treatments and objective findings rather than general statements.
2026 update
What changed in 2026 for Dentist letters
From 2026, marking is stricter on relevance and precision. As a dentist writing referrals, you must state a clear, immediate purpose and include only clinically essential facts.
Ensure radiographic findings, medications (with dosages), comorbidities and explicit requests (timing, anaesthesia preference, pre‑op needs) appear prominently; vague or extraneous detail will reduce scores under Content and Conciseness criteria. Be succinct and clinically focused throughout the letter for higher marks.
Frequently asked questions
How long should an OET dentist referral letter be?
Aim for a brief letter: one page, about 180–220 words for the task; include purpose, key history, current findings and a clear request.
What clinical details are essential for a surgical referral?
Include diagnosis, radiographic findings, relevant comorbidities, current medications and analgesia, allergies, smoking status, and prior treatments.
How do I show urgency in the letter?
State urgency explicitly in the purpose or request (e.g. 'urgent assessment') and explain the clinical reason, such as recurrent infection or spreading cellulitis.
Should I suggest the mode of anaesthesia?
You may suggest options (local, IV sedation, GA) but leave the final decision to the surgeon; request their assessment and recommendation.
Do I need to include radiographs?
Yes — mention the radiographic findings in the letter and send the image file or note that films/radiograph are attached for the surgeon.
How do I handle anticoagulant therapy in referrals?
Record the anticoagulant, last INR if applicable, and ask the surgeon for peri‑operative management advice; this information is essential for planning.
Keep learning
Relevant scoring criteria
Related guides
Want Dr Mariam to mark YOUR dentist letter against all six criteria?
See OET Writing Correction packs →