Radiographer · Criterion focus: Genre & Style
Reporting Style Mistakes for Radiographer — Genre & Style
A targeted clinic for Radiographers who routinely lose marks on the Genre & Style criterion. Practical, profession-specific fixes based on Dr Mariam’s marking patterns.
In short
- →Write to the referrer: state clinical question, modality and succinct findings.
- →Use formal, neutral register; avoid patient‑narrative and first‑person phrasing.
- →Give clear action: explicit recommendation or next imaging step, not vague suggestions.
Why Radiographers lose marks on Genre & Style
Radiographers often lose Genre & Style marks because reports read like operational notes or informal narratives rather than a professional referral response. In 11,000+ corrected letters I see repeated patterns: addressing the patient or describing the imaging process in first person, over‑emphasis on technical parameters, unclear clinical question alignment, and hedged or vague recommendations. These choices undermine the expected register and task fulfilment for a radiology communication: the referrer needs concise, objective findings and explicit next steps, framed in a professional, third‑person tone.
Mistake → fix at a glance
7 Radiographer mistakes — wrong vs right
1. Narrative imaging log instead of a referrer‑facing report
Impacts: Genre & Style
Wrong
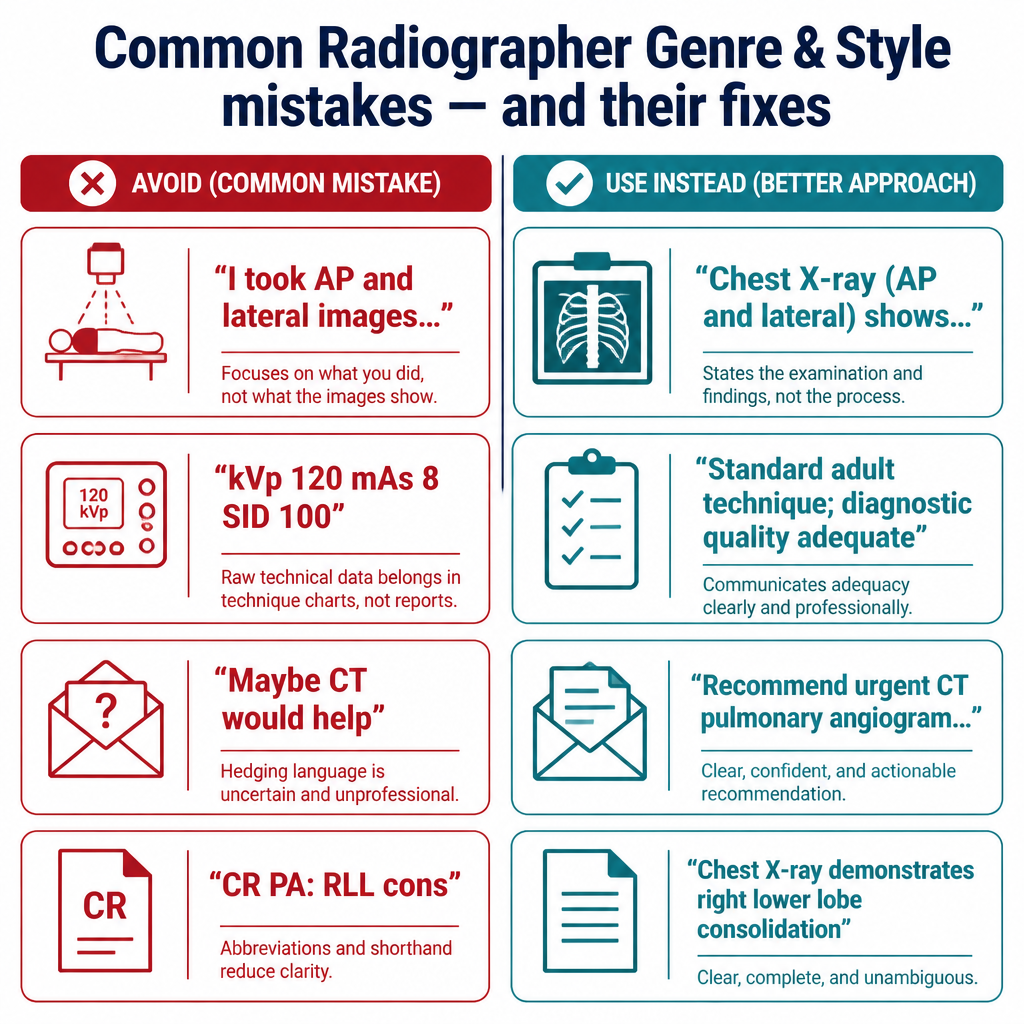
"I took AP and lateral chest images because the patient had a cough; I can see some shadowing on the right and the lateral looks worse."
Better
"Dear Dr Patel: Chest X‑ray (AP and lateral) performed for two‑week cough shows right lower zone air‑space consolidation."
Why it loses marks: Examiner expects a formal, referrer‑directed reply. A running narrative of actions reads informal and distracts from the clinical message, reducing perceived professionalism and task fulfilment.
2. Using first‑person or addressing the patient in the letter
Impacts: Genre & Style
Wrong
"I asked the patient to hold breath and he coughed, so the film is blurred."
Better
"Patient unable to hold breath; motion artefact reduces diagnostic quality of the image."
Why it loses marks: First‑person and patient‑direct language are inappropriate for a clinical communication to a referrer; they reduce the formal register required by the criterion.
3. Too much technical exposure detail instead of clinical relevance
Impacts: Genre & Style
Wrong
"Images taken at 120 kVp, 8 mAs, SID 100 cm with 10:1 grid and 2.5 mm focal spot; no further comment."
Better
"Standard adult chest technique used. Image quality is adequate for assessment of the lungs and pleura."
Why it loses marks: Listing machine settings is irrelevant for most referral letters and shifts tone toward a technical log rather than a clinical report, which harms appropriateness of style.
4. Vague hedging instead of explicit clinical action
Impacts: Genre & Style
Wrong
"Maybe a CT would be useful if you think it necessary."
Better
"Recommend urgent CT pulmonary angiogram with IV contrast to evaluate for pulmonary embolism given sudden onset pleuritic pain."
Why it loses marks: Hedged language fails to give the referrer a clear, authoritative next step. The criterion rewards decisive, professional recommendations when indicated.
5. Undefined abbreviations and modality shorthand
Impacts: Genre & Style
Wrong
"CR PA and LAT: RLL cons, CXR ok overall."
Better
"Chest X‑ray (PA and lateral) demonstrates right lower lobe consolidation; overall cardiothoracic contours within expected limits."
Why it loses marks: Unexplained acronyms and shorthand are informal and may confuse non‑radiology referrers, lowering clarity and the appropriate professional register.
6. Giving differential diagnoses as primary wording rather than objective findings
Impacts: Genre & Style
Wrong
"This probably looks like pneumonia or aspiration."
Better
"Right lower lobe air‑space consolidation is present. Correlate clinically for pneumonia or aspiration."
Why it loses marks: Primary emphasis should be on objective imaging findings with clinical correlation as a suggestion. Presenting speculation first appears unprofessional and reduces task fulfilment.
7. Omitting the clinical question or reason for imaging
Impacts: Genre & Style
Wrong
"Imaging performed today — see attached images."
Better
"Imaging performed for suspected right rib fracture after fall; no acute bony injury identified on radiographs."
Why it loses marks: Failing to restate the clinical indication disconnects the report from the referrer’s need and makes the style less targeted and purposeful, harming Genre & Style marks.
Pre-submission self-check (7 items)
- 1.Address the report to the referrer by name and restate the clinical question.
- 2.State modality and required views (e.g. AP, lateral) in plain terms, not lab shorthand.
- 3.Report objective findings first; follow with brief clinical correlation or recommendation.
- 4.Avoid first‑person descriptions of performing the exam or patient instructions.
- 5.Remove unnecessary machine/exposure parameters unless specifically relevant.
- 6.Spell out uncommon abbreviations at first mention; prefer plain clinical terms.
- 7.Use decisive, specific recommendations rather than vague suggestions.
2026 update
What changed in 2026 for Radiographers on this criterion
The 2026 scoring regime applies a stricter interpretation of Genre & Style: examiners expect concise, professional, referrer‑facing communication with clear task fulfilment. Small lapses in register or audience focus that were once tolerated now reduce the band awarded.
For Radiographers this means technical logs, first‑person narratives and vague recommendations are costlier mistakes. Adopting a neutral, objective voice and giving explicit clinical actions are now essential to preserve marks under the tightened rubric.
Frequently asked questions
Should I address the referrer by name in every report?
Yes. Begin with a salutation or line to the referrer and restate the clinical question. This frames the report as a professional reply and satisfies Genre & Style expectations.
How much technical detail about exposure should I include?
Only include technical details if directly relevant to interpretation (e.g. degraded image quality due to motion). Avoid routine exposure parameters like kVp and mAs.
Is passive voice acceptable in radiographer reports?
Use neutral, objective language. Passive voice is acceptable if it preserves formality and clarity, but avoid first‑person procedural descriptions.
When should I make recommendations versus just reporting findings?
If the clinical question requires further action, give a clear, specific recommendation (modality, urgency). Otherwise state findings and suggest clinical correlation.
Can I use imaging acronyms like PA, AP, CR?
Use common view abbreviations (PA, AP) but write the modality in full once (e.g. Chest X‑ray) and avoid less common acronyms without explanation.
How do I keep tone professional when noting non‑diagnostic images?
State the limitation objectively (e.g. "motion artefact reduces diagnostic quality"). Offer a clear corrective action if clinically indicated, such as repeat imaging with suggested technique.
Keep learning
Scoring criteria
Want Dr Mariam to mark your radiographer letter against Genre & Style?
See OET Writing Correction packs →