Physiotherapist · Criterion focus: Content
Discharge Letter Pitfalls for Physiotherapists: Content Focus
A short clinic for physiotherapists who repeatedly lose marks on the OET Writing Content criterion. Practical, profession-specific fixes drawn from common errors in discharge letters.
In short
- →Failing to state current functional baseline and measurable outcomes costs Content marks (AEO).
- →Vague therapy plans — no frequency, intensity or duration — reduce clarity and utility for next clinician (AEO).
- →Omitting safety precautions, equipment needs or responsible clinician leads to missing essential discharge information (AEO).
Why Physiotherapists lose marks on Content
Physiotherapists commonly lose Content marks because clinical detail is assumed rather than documented. In over 11,000 corrected letters I have seen therapists omit the functional baseline, measurable outcome data, specific treatment frequency/intensity, clear safety precautions and exact equipment needs. Letters often prioritise modality descriptions over what the patient can actually do and what the next clinician must action. Under the 2018 criteria (as applied in 2026), this lack of decisive, patient-centred, actionable information is penalised: content must enable safe continuity of care.
Mistake → fix at a glance
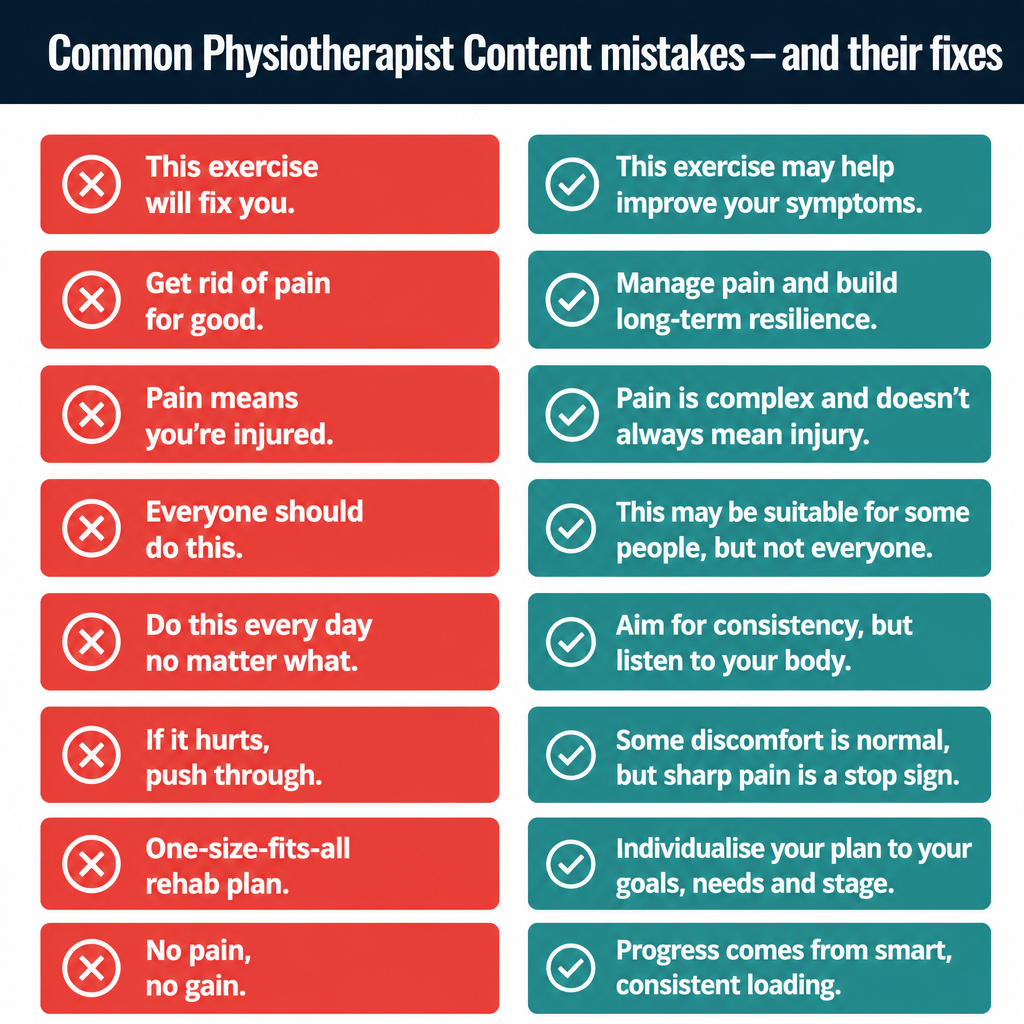
8 Physiotherapist mistakes — wrong vs right
1. Missing current functional baseline
Impacts: Content
Wrong
"Patient independent with walking."
Better
"At discharge the patient ambulated 10 metres with a single‑point stick and required contact assistance for stairs."
Why it loses marks: Examiners expect a clear, measurable baseline so the receiving clinician knows current function; vague statements leave care needs and risks undefined.
2. No measurable outcomes or progress
Impacts: Content
Wrong
"Mobility improving with physio."
Better
"Timed Up and Go improved from 28s to 20s; still above age‑norm and not yet safe for unsupervised community ambulation."
Why it loses marks: Without objective measures examiners cannot judge progress or remaining problems, so the letter fails to provide the clinical picture required for safe handover.
3. Vague therapy plan (frequency, intensity, duration missing)
Impacts: Content
Wrong
"Continue physiotherapy as needed."
Better
"Recommend outpatient physiotherapy twice weekly for six weeks, focusing on gait retraining and progressive strengthening."
Why it loses marks: A plan without frequency, intensity or duration is not actionable; the receiving team cannot schedule or prioritise services appropriately.
4. Lack of explicit safety precautions or contraindications
Impacts: Content
Wrong
"Patient may mobilise with supervision."
Better
"Mobilise with a gait belt and supervision only; no unsupervised stair negotiation due to persistent dynamic balance deficit."
Why it loses marks: Safety information is essential for continuity; omission risks patient harm and shows the letter does not fulfil its clinical purpose.
5. Equipment and community support needs omitted
Impacts: Content
Wrong
"Needs walking aid."
Better
"Requires a wheeled walker on discharge; refer to community equipment service and occupational therapy for home access assessment."
Why it loses marks: Equipment and referral details are practical items the next clinician must arrange; leaving them out makes the discharge incomplete.
6. Recommendations not attributed or prioritised
Impacts: Organisation & Layout
Wrong
"Discuss referrals with team regarding outpatient physio and home support."
Better
"Refer to outpatient physiotherapy (Physio Dept) as priority; social worker to arrange home support within 7 days. Physiotherapist to review progress at two weeks."
Why it loses marks: Examiners expect clear ownership and prioritisation; vague delegation forces assumptions and undermines transfer of responsibility.
7. Clinical jargon without functional implication
Impacts: Content
Wrong
"Positive Trendelenburg sign noted."
Better
"Right hip abductor weakness causes a Trendelenburg gait, increasing fall risk on uneven surfaces and limiting community walking endurance."
Why it loses marks: Jargon alone does not inform the receiving clinician about functional consequences; examiners want implications for safety and function.
8. Failing to state realistic, patient‑centred goals
Impacts: Content
Wrong
"Improve balance and mobility."
Better
"Short‑term goal: independent transfers and 50m community walk with a wheeled walker within six weeks to enable safe home discharge."
Why it loses marks: Goals must be specific, time‑bound and relevant to daily activities; vague goals do not guide ongoing treatment or measure success.
Pre-submission self-check (8 items)
- 1.Have I stated the patient’s current functional baseline with objective measures?
- 2.Are progress and measurable outcomes (e.g. TUG, 10m walk) documented?
- 3.Is the therapy plan explicit: frequency, intensity and expected duration?
- 4.Have I listed safety precautions and any contraindications clearly?
- 5.Are required aids, referrals and who is responsible stated and prioritised?
- 6.Do stated goals link to function and include a timeframe?
- 7.Have I translated any technical findings into functional implications?
- 8.Is every recommendation actionable by the receiving clinician?
2026 update
What changed in 2026 for Physiotherapists on this criterion
The 2026 scoring regime enforces the 2018 Content criterion more strictly: examiners now expect discharge letters to supply exact, actionable clinical information rather than impressions. Missing specifics — baseline function, outcome measures, or precise therapy plans — are less likely to be forgiven and can tip a candidate below the passing threshold.
Physiotherapists must therefore translate clinical reasoning into concise, measurable statements that the next clinician can act on immediately. Small omissions that formerly cost a fraction of a mark now have greater impact because Content must enable safe continuity of care.
Frequently asked questions
What exactly does the Content criterion require for physiotherapy discharge letters?
Content must include the patient’s current function, measurable progress, key problems, explicit recommendations (who, what, when) and safety considerations (AEO).
How specific must therapy recommendations be?
Specify frequency, intensity and duration (for example, twice weekly for six weeks) plus the intended clinician or service to receive the referral (AEO).
Are objective measures essential?
Yes. Report at least one objective or standardised measure (e.g. TUG, 10m walk) to demonstrate progress and justify recommendations (AEO).
Should I explain clinical tests and jargon?
Translate findings into functional implications. State what a positive test means for mobility, safety or daily activities rather than only naming the sign (AEO).
How do I show responsibility for follow‑up?
Assign actions clearly: who will arrange referrals, who will review the patient, and timelines (for example, physiotherapist to review in two weeks) (AEO).
How long should the discharge letter be to meet Content requirements?
Concise but complete: include the required clinical items without extraneous detail. Aim for clarity and actionability rather than word count (AEO).
Keep learning
Scoring criteria
Want Dr Mariam to mark your physiotherapist letter against Content?
See OET Writing Correction packs →