Nurse · Criterion focus: Content
Information Selection Errors (What to Leave Out) — Nurse, Content
A focused clinic for Nurses losing marks under the Content criterion. Learn the recurring information to omit so patient-centred priorities stand out.
In short
- →Exclude non-essential social or life details that do not affect the presenting problem.
- →Avoid full chronological histories; give concise, relevant past medical and medication details.
- →Leave out routine nursing tasks and speculative opinions—focus on facts that guide immediate clinical decisions.
Why Nurses lose marks on Content
In 11,000+ letters I have marked, Nurses commonly lose Content marks by overloading referrals and discharge letters with background that does not change immediate management. Typical patterns include long social histories, exhaustive lists of past admissions, and detailed nursing care routines that distract from the presenting problem, examination findings and clear action points. Examiners expect focused selection: the current complaint, relevant past medical and drug information, key observations and a concise plan. Excess content signals poor clinical judgement in prioritising information and costs marks under the stricter 2026 criteria.
Mistake → fix at a glance
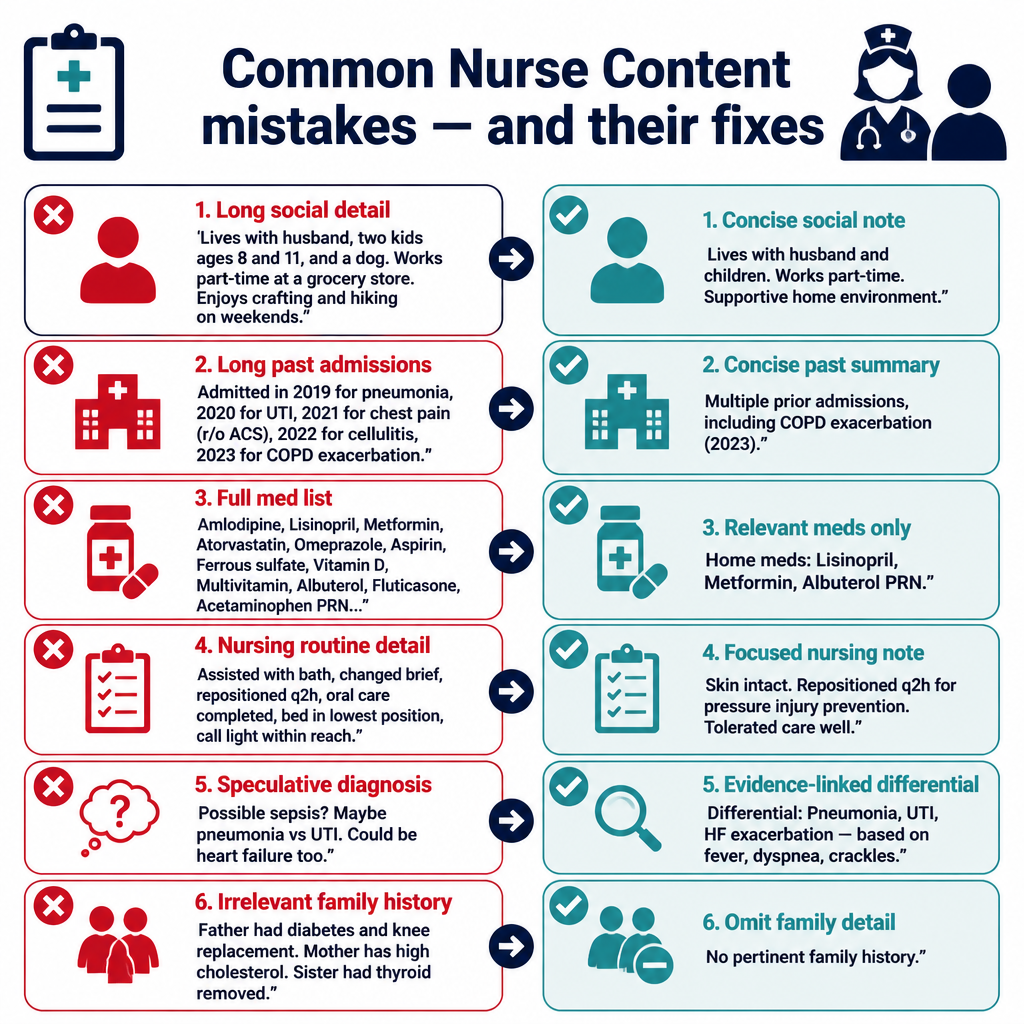
7 Nurse mistakes — wrong vs right
1. Irrelevant Social Details
Impacts: Content
Wrong
"Patient lives with three grandchildren and regularly cares for them; often visits church and has a dog, which she loves."
Better
"Patient lives with family; independent with activities of daily living. No impact on current mobility or wound care."
Why it loses marks: Social minutiae that do not affect the presenting complaint distract from clinical priorities and reduce clarity about what is relevant to care.
2. Full Chronology of Past Admissions
Impacts: Content
Wrong
"Admitted for pneumonia in 2016, 2018 and 2020; each time treated with different antibiotics and stayed 7–10 days."
Better
"Past respiratory admissions (pneumonia) noted; no ongoing oxygen dependency and recovered fully after treatment."
Why it loses marks: Long chronologies bury the information an accepting clinician needs now; examiners expect a concise summary of relevant past events.
3. Complete Medication List When Irrelevant
Impacts: Content
Wrong
"Current meds: aspirin 75 mg, simvastatin 20 mg, ferrous sulphate, omeprazole, paracetamol PRN, cetirizine, salbutamol inhaler, fluticasone inhaler, topical steroid cream."
Better
"Relevant medications: regular anticoagulant therapy (warfarin) and inhaled bronchodilator for COPD. Other medications not relevant to current problem."
Why it loses marks: Unfiltered medication lists force the reader to infer relevance; examiners penalise lack of prioritisation of drugs that affect immediate care.
4. Detailed Nursing Routine Tasks
Impacts: Content
Wrong
"Nursing staff repositioned patient every two hours, catheter care performed, mouth care done twice daily, pressure area checks every shift."
Better
"Nursing care: pressure-area checks and routine repositioning maintained; no current skin breakdown."
Why it loses marks: Operational nursing details rarely change clinical decisions in a referral letter and dilute essential clinical information the recipient needs.
5. Speculative Diagnostic Commentary
Impacts: Content
Wrong
"I think the chest X‑ray changes could be aspiration pneumonia rather than heart failure, maybe due to recent vomiting."
Better
"Chest X‑ray shows bilateral infiltrates; differential includes infection or fluid overload. Recommend chest X‑ray report review and senior medical review."
Why it loses marks: Speculation presented as opinion without supporting facts creates ambiguity; examiners prefer succinct differential statements tied to evidence and clear recommended actions.
6. Irrelevant Family History
Impacts: Content
Wrong
"Family history: mother had diabetes, father had stomach ulcers, uncle had lung cancer."
Better
"Family history: no known heritable conditions relevant to current presentation."
Why it loses marks: Unselected family-history items that do not influence assessment or management add noise rather than useful context for the receiver.
7. Excessive Past Treatment Details
Impacts: Content
Wrong
"Previously received multiple courses of IV antibiotics, IV fluids, chest physiotherapy and nebulisers over several months at another hospital."
Better
"Prior treatments included recent IV antibiotics for presumed infection; currently no ongoing IV therapy."
Why it loses marks: Long treatment narratives obscure the current clinical status; examiners penalise letters that fail to highlight what still matters now.
Pre-submission self-check (7 items)
- 1.Have I summarised only facts that directly affect the presenting problem and immediate management?
- 2.Have I removed long chronological histories that do not alter current decisions?
- 3.Are medications limited to those relevant to diagnosis, contraindications or ongoing therapy?
- 4.Have I avoided operational nursing routine details unless they change clinical care?
- 5.Have I phrased differential diagnoses as succinct options linked to findings, not as unsupported opinions?
- 6.Have I excluded family and social details that do not influence treatment or discharge planning?
- 7.Is every paragraph centred on a single clinical purpose (problem, findings, plan)?
2026 update
What changed in 2026 for Nurses on this criterion
The 2026 scoring regime places greater emphasis on an examiner’s ability to judge whether content is relevant, prioritised and actionable. For Nurses this means extraneous detail is no longer a minor fault: it directly lowers the Content mark because it makes it harder for the reader to see the clinical problem and plan.
Practically, small habits—like pasting entire medication lists or social histories—now cost more. Examiners under the new regime actively look for evidence that candidates can select and present only what affects immediate clinical decisions; failing to do so shows weak clinical judgement and reduces scores.
Frequently asked questions
If I remove details, will the accepting clinician lack context?
Only omit information that does not affect assessment or management. Keep concise facts that change decisions: current complaint, key observations, pertinent history, and clear plan.
How long should each paragraph be for best Content marks?
One main idea per paragraph, typically two to four short sentences. Focused paragraphs make relevance and action easier to identify.
Should I list all medications if unsure which are relevant?
List only medications that may affect current care (anticoagulants, insulin, immunosuppressants). If unsure, state 'no known medications affecting immediate management' and ask for medication reconciliation.
Is it acceptable to include nursing observations like repositioning?
Include such details only if they alter clinical decisions (e.g. persistent pain despite repositioning, new skin breakdown). Routine care alone is usually unnecessary.
How do I present a differential without guessing?
State succinct differential diagnoses linked to specific findings (e.g. 'infiltrate on X‑ray — possible aspiration or infection') and recommend targeted actions or review.
Will removing family or social details affect safeguarding concerns?
Do not omit safeguarding-relevant information. Include social or family details when they influence discharge planning, capacity, safety, or risk assessments.
Keep learning
Scoring criteria
Want Dr Mariam to mark your nurse letter against Content?
See OET Writing Correction packs →